| Weight | 1 lbs |
|---|---|
| Dimensions | 9 × 5 × 2 in |
| host | mouse |
| isotype | IgG |
| clonality | monoclonal |
| concentration | concentrate, predilute |
| applications | IHC |
| reactivity | human |
| available size | 0.1 mL, 0.5 mL, 1 mL concentrated, 7 mL prediluted |

rabbit anti-MSH-2 monoclonal antibody (ZR260) 6430
Price range: $160.00 through $528.00
Antibody summary
- Rabbit monoclonal to MSH-2
- Suitable for: Immunohistochemistry (formalin-fixed, paraffin-embedded tissues)
- Reacts with: Human
- Isotype:IgG
- Control: Colon carcinoma
- Visualization: Nuclear
- 0.1, 0.5, 1.0 mL concentrated, 7 mL prediluted
rabbit anti-MSH-2 monoclonal antibody ZR260 6430
| target relevance |
|---|
| Homo sapiens MSH2 DNA mismatch repair protein Msh2 |
| Protein names DNA mismatch repair protein Msh2 |
| Alternative names MutS protein homolog 2 |
| Gene names MSH2 |
| Protein family Belongs to the DNA mismatch repair MutS family |
| Function Component of the post-replicative DNA mismatch repair system (MMR). Forms two different heterodimers: MutS alpha (MSH2-MSH6 heterodimer) and MutS beta (MSH2-MSH3 heterodimer) which binds to DNA mismatches thereby initiating DNA repair. When bound, heterodimers bend the DNA helix and shields approximately 20 base pairs. MutS alpha recognizes single base mismatches and dinucleotide insertion-deletion loops (IDL) in the DNA. MutS beta recognizes larger insertion-deletion loops up to 13 nucleotides long. After mismatch binding, MutS alpha or beta forms a ternary complex with the MutL alpha heterodimer, which is thought to be responsible for directing the downstream MMR events, including strand discrimination, excision, and resynthesis. Recruits DNA helicase MCM9 to chromatin which unwinds the mismatch containing DNA strand (PubMed:26300262). ATP binding and hydrolysis play a pivotal role in mismatch repair functions. The ATPase activity associated with MutS alpha regulates binding similar to a molecular switch: mismatched DNA provokes ADP-->ATP exchange, resulting in a discernible conformational transition that converts MutS alpha into a sliding clamp capable of hydrolysis-independent diffusion along the DNA backbone. This transition is crucial for mismatch repair. MutS alpha may also play a role in DNA homologous recombination repair. In melanocytes may modulate both UV-B-induced cell cycle regulation and apoptosis |
| Subcellular location Nucleus, Chromosome |
| Structure Component of the DNA mismatch repair (MMR) complex composed at least of MSH2, MSH3, MSH6, PMS1 and MLH1 (PubMed:26300262). Heterodimer consisting of MSH2-MSH6 (MutS alpha) or MSH2-MSH3 (MutS beta) (PubMed:8942985). Both heterodimers form a ternary complex with MutL alpha (MLH1-PMS1) (PubMed:10856833, PubMed:11427529, PubMed:11429708, PubMed:12414623, PubMed:14676842, PubMed:9788596). Interacts with MCM9; the interaction recruits MCM9 to chromatin (PubMed:26300262). Interacts with MCM8 (PubMed:26300262). Interacts with EXO1 (PubMed:10856833, PubMed:11427529, PubMed:11429708, PubMed:12414623, PubMed:14676842, PubMed:9788596). Part of the BRCA1-associated genome surveillance complex (BASC), which contains BRCA1, MSH2, MSH6, MLH1, ATM, BLM, PMS2 and the RAD50-MRE11-NBS1 protein complex (PubMed:10783165). This association could be a dynamic process changing throughout the cell cycle and within subnuclear domains (PubMed:10783165). Interacts with ATR (PubMed:14657349). Interacts with SLX4/BTBD12; this interaction is direct and links MutS beta to SLX4, a subunit of different structure-specific endonucleases (PubMed:19596235). Interacts with SMARCAD1 (PubMed:18675275) |
| Post-translational modification Phosphorylated by PRKCZ, which may prevent MutS alpha degradation by the ubiquitin-proteasome pathway Sequentially deacetylated and polyubiquitinated by HDAC6, leading to MSH2 degradation |
| Involvement in disease Lynch syndrome 1 A form of Lynch syndrome, an autosomal dominant disease associated with marked increase in cancer susceptibility. It is characterized by a familial predisposition to early-onset colorectal carcinoma (CRC) and extra-colonic tumors of the gastrointestinal, urological and female reproductive tracts. Lynch syndrome is reported to be the most common form of inherited colorectal cancer in the Western world. Clinically, it is often divided into two subgroups. Type I is characterized by hereditary predisposition to colorectal cancer, a young age of onset, and carcinoma observed in the proximal colon. Type II is characterized by increased risk for cancers in certain tissues such as the uterus, ovary, breast, stomach, small intestine, skin, and larynx in addition to the colon. Diagnosis of classical Lynch syndrome is based on the Amsterdam criteria: 3 or more relatives affected by colorectal cancer, one a first degree relative of the other two; 2 or more generation affected; 1 or more colorectal cancers presenting before 50 years of age; exclusion of hereditary polyposis syndromes. The term 'suspected Lynch syndrome' or 'incomplete Lynch syndrome' can be used to describe families who do not or only partially fulfill the Amsterdam criteria, but in whom a genetic basis for colon cancer is strongly suspected. Muir-Torre syndrome Rare autosomal dominant disorder characterized by sebaceous neoplasms and visceral malignancy. Endometrial cancer A malignancy of endometrium, the mucous lining of the uterus. Most endometrial cancers are adenocarcinomas, cancers that begin in cells that make and release mucus and other fluids. Mismatch repair cancer syndrome 2 An autosomal recessive form of mismatch repair cancer syndrome, a childhood cancer predisposition syndrome encompassing a broad tumor spectrum. This includes hematological malignancies, central nervous system tumors, Lynch syndrome-associated malignancies such as colorectal tumors as well as multiple intestinal polyps, embryonic tumors and rhabdomyosarcoma. Multiple cafe-au-lait macules, a feature reminiscent of neurofibromatosis type 1, are often found as first manifestation of the underlying cancer. Colorectal cancer A complex disease characterized by malignant lesions arising from the inner wall of the large intestine (the colon) and the rectum. Genetic alterations are often associated with progression from premalignant lesion (adenoma) to invasive adenocarcinoma. Risk factors for cancer of the colon and rectum include colon polyps, long-standing ulcerative colitis, and genetic family history. |
| Keywords 3D-structure, Acetylation, Alternative splicing, ATP-binding, Chromosome, Disease variant, DNA damage, DNA repair, DNA-binding, Hereditary nonpolyposis colorectal cancer, Isopeptide bond, Nucleotide-binding, Nucleus, Phosphoprotein, Proteomics identification, Reference proteome, Tumor suppressor, Ubl conjugation |
| Sequence MAVQPKETLQLESAAEVGFVRFFQGMPEKPTTTVRLFDRGDFYTAHGEDALLAAREVFKT QGVIKYMGPAGAKNLQSVVLSKMNFESFVKDLLLVRQYRVEVYKNRAGNKASKENDWYLA YKASPGNLSQFEDILFGNNDMSASIGVVGVKMSAVDGQRQVGVGYVDSIQRKLGLCEFPD NDQFSNLEALLIQIGPKECVLPGGETAGDMGKLRQIIQRGGILITERKKADFSTKDIYQD LNRLLKGKKGEQMNSAVLPEMENQVAVSSLSAVIKFLELLSDDSNFGQFELTTFDFSQYM KLDIAAVRALNLFQGSVEDTTGSQSLAALLNKCKTPQGQRLVNQWIKQPLMDKNRIEERL NLVEAFVEDAELRQTLQEDLLRRFPDLNRLAKKFQRQAANLQDCYRLYQGINQLPNVIQA LEKHEGKHQKLLLAVFVTPLTDLRSDFSKFQEMIETTLDMDQVENHEFLVKPSFDPNLSE LREIMNDLEKKMQSTLISAARDLGLDPGKQIKLDSSAQFGYYFRVTCKEEKVLRNNKNFS TVDIQKNGVKFTNSKLTSLNEEYTKNKTEYEEAQDAIVKEIVNISSGYVEPMQTLNDVLA QLDAVVSFAHVSNGAPVPYVRPAILEKGQGRIILKASRHACVEVQDEIAFIPNDVYFEKD KQMFHIITGPNMGGKSTYIRQTGVIVLMAQIGCFVPCESAEVSIVDCILARVGAGDSQLK GVSTFMAEMLETASILRSATKDSLIIIDELGRGTSTYDGFGLAWAISEYIATKIGAFCMF ATHFHELTALANQIPTVNNLHVTALTTEETLTMLYQVKKGVCDQSFGIHVAELANFPKHV IECAKQKALELEEFQYIGESQGYDIMEPAAKKCYLEREQGEKIIQEFLSKVKQMPFTEMS EENITIKLKQLKAEVIAKNNSFVNEIISRIKVTT |
| UniProt accession: P43246 |
Data
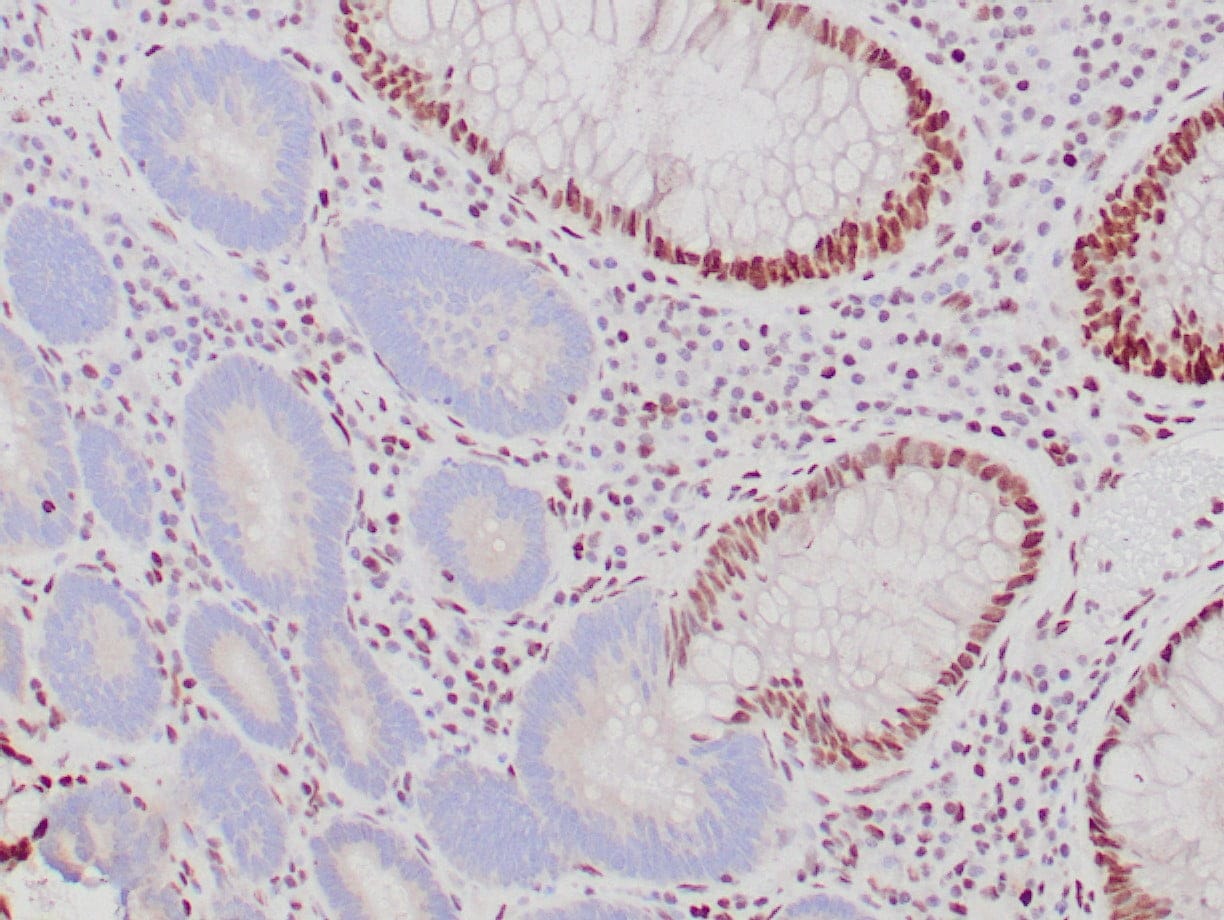 |
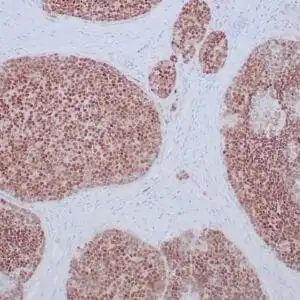
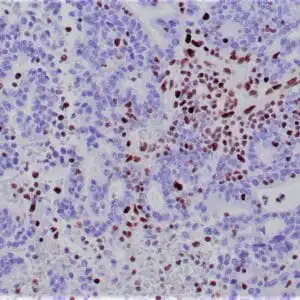
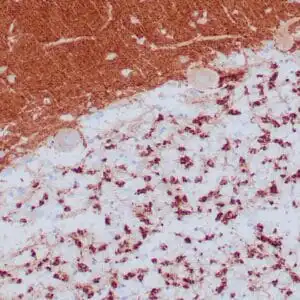
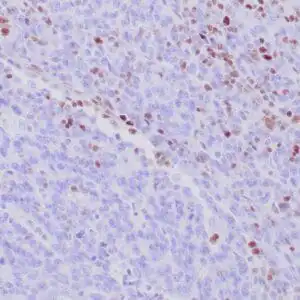
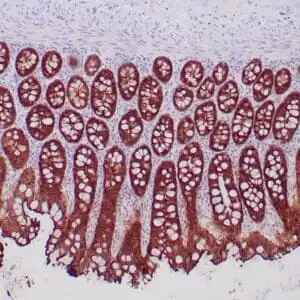
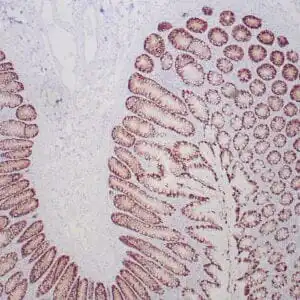
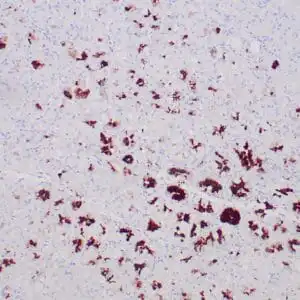
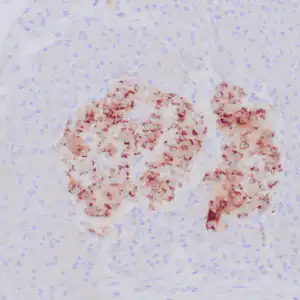
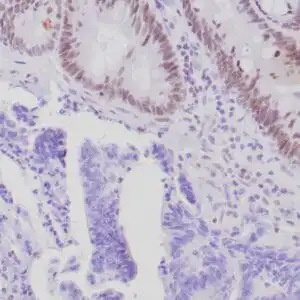
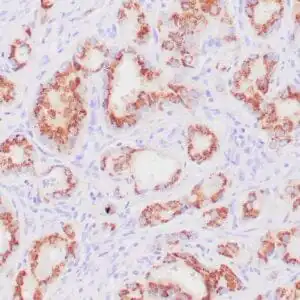
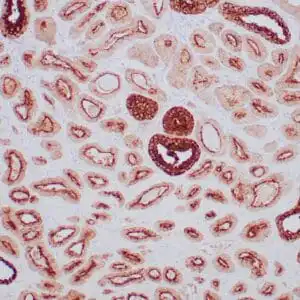
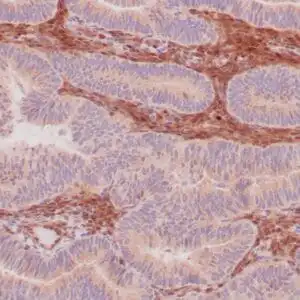
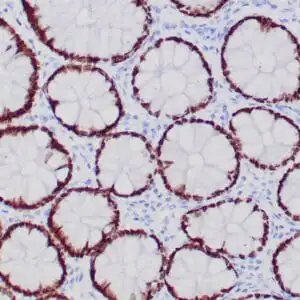
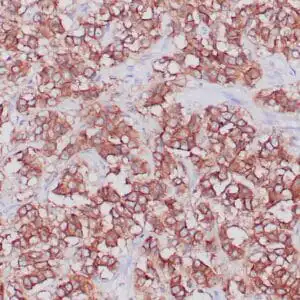
| Formalin-fixed, paraffin-embedded human colon adenocarcinoma stained with anti-MSH-2 antibody using peroxidase-conjugate and DAB chromogen. Note the absence nuclear staining of tumor cells and the presence of nuclear staining of normal mucosa |
FAQ & Publications
Frequently Asked Questions
What species does the rabbit anti-MSH-2 monoclonal antibody (ZR260) specifically react with?
This monoclonal antibody specifically reacts with human MSH-2 protein.
Which applications is the rabbit anti-MSH-2 monoclonal antibody (ZR260) validated for?
It is suitable and tested for Immunohistochemistry (IHC) on formalin-fixed, paraffin-embedded tissues.
What are the recommended storage conditions for maintaining the stability of this antibody?
For short-term storage, keep the antibody at 2-8°C, and for longer-term storage, freeze at -20°C while avoiding repeated freeze/thaw cycles.
Publications
| pmid | title | authors | citation |
|---|---|---|---|
| We haven't added any publications to our database yet. | |||
Published literature highly relevant to the biological target of this product and referencing this antibody or clone are retrieved from the PubMed database provided by the United States National Library of Medicine at the National Institutes of Health.
Protocols
| relevant to this product |
|---|
| IHC |
Documents
| Batch Number | QC File | SDS |
|---|---|---|
| To view batch-specific Safety Datasheets and Quality Certificates associated with your account, please Log In. | ||
Only logged in customers who have purchased this product may leave a review.

Reviews
There are no reviews yet.